Dashboard views should be the rule rather than the exception in EHR design
Physicians and nurses have to deal with complex data involving a number of realms, making quick judgments based on the overview of the patient's story.

Dashboards beat nested navigation in several ways:
Physicians and nurses have to deal with complex data involving a number of realms, making quick judgments based on the overview of the patient's story.
Dashboards beat nested navigation in several ways:
- They minimize navigation.
- They reduce cognitive load by presenting the needed information in a single view.
- Users don't have to think "What next? Where next?
- Users don't have to use visual memory to recall the last page view: "What was that potassium value I saw seconds ago? Was that drug dose once a day or twice day?"
- Users can "scan the scene" to quickly see if there are any abnormals. If the view is "clean", then we can move on.
- They accommodate a variety of workflow styles. Methodical or meandering paths work equally well when only the eye (and not the finger) does the walking. ABCDE sequence is as easy as AEDCB.
- They can be customized or personalized to meet unique user needs.
There are some caveats.
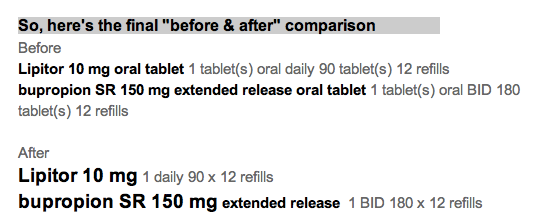
- Provide only the information needed for the tasks at hand. No more, and no less. That may mean leaving out detail from the grand view, while making that detail available when drilling down.
- Use visual cues. They don't have to be words. They do need to be recognizable at a glance. Think icons and traffic lights.
- Try the designs out on real world users.