
I did a closing keynote presentation for HIMSS Virtual Conference today on EMR Usability. Here are the visuals, without my soothing voice.
View more presentations from University of Missouri Health Care.
Family physician & usability evangelist Jeff Belden MD
writes about EHR usability & data visualization at the point of care.
I just finished writing a white paper for HIMSS titled "Defining and Testing EMR Usability: Principles and Proposed Methods of EMR Usability Evaluation and Rating". It's publicly available at this link.
It has been a great team to work with. Many thanks to my Human-Computer Interaction co-authors, Rebecca Grayson and Janey Barnes. They brought experience with clinical systems and their body of user-centered design knowledge to the task. Thanks also to the team leaders Penn White MD and Tiana Thomas for harnessing the power of a cadre of volunteer contributors to the effort.
Briefly, this paper describes how poor EMR usability has hindered user adoption among physicians and hospitals. We describe a number of usability principles that apply to EMRs in particular, and then offer evaluation and testing methods for finished EMR products, and suggest ways to rate the EMRs.
Our hope is that certifying and rating organizations such as Certification Commission for Healthcare Information Technology (CCHIT) or the American Academy of Family Physicians (AAFP) will be able to use this work in developing their own rating methods that can help EMR purchasers.
I love this line.
It's the title of one of my favorite books on software usability, written by Steve Krug.
The human-computer interaction pros refer to this principle as "reducing cognitive load." Don't waste precious brain resources on stuff the application should be able to do quickly, accurately, and invisibly.
Here's a prime example.
In displaying lab results, why not do the math for the clinician user? Don't make me calculate how long ago the last lab result was obtained. Tell me it was about 2 weeks ago. The precision can get more relaxed the longer ago the result was obtained.
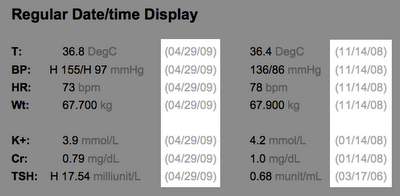

The same principle applies to displaying the patient's age. Don't just show me the date of birth. Do the math for me.
I have plenty of more important things to think about.
Most clinicians I know suffer from "alert fatigue". I don't mean they feel tired from too much caffeine.
I mean, they are tired of EHR software crying wolf with too many drug interaction warnings. Embattled users simply dismiss all drug interaction warnings without reading them. Mild or theoretical interactions should be suppressable by individual user preference, as a default setting.
This is a significant patient safety issue.
If I am relying on my software to warn me about serious drug interactions, then the warnings about milder or dubious interactions are annoying, distracting false alarms. I need to be aware of serious interactions, so I can adjust therapy.
Here's another problem: I get warned that drug A interacts with drug B. I dismiss the warning. Then I immediately get warned that drug B interacts with drug A. I know that!
Worse yet, if I then change the dose of drug A, I get warned all over again. We need smarter systems now, geared to what fallable, imperfect, tired human users need, and geared to keeping patients safe.
Here is a modest proposal of a way to display drug interactions.

Note that the key findings are in the middle, the drug names are prominent, the severity level is great big number, and user pref settings are right there.

We are being freed from the document-centric mental model of the medical record. In the paper past, we only could create, save, read, and review paper documents. That has changed, but our way of thinking has not.
As with data tables that allow us to sort, or links that allow us to drill down, our clinical documents have interactive features. Or should have.
So let me propose a model for the Four-Layer EMR. It would use some kind of "hide/reveal" technology. Show me the level of detail I, the reader, need right now, in this context.

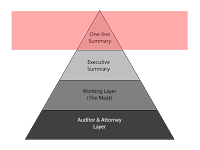
The top layer I call the "one-line summary". What few words characterize this encounter. I am thinking of ambulatory physician visits. Perhaps other readers can translate this into other kinds of clinical encounters.
The one-line summary would be a terse description like: "diabetes, A1C 8.2, start metformin 500 BID" or "acute sinusitis > amoxicillin 875 BID 7 days" or "well woman exam > Gardisil, Yasmin".
The benefit? I can look at a list of all the visits chronologically and see what happened.
Like this:
Brenda Star Acct No: 309144869
02/11/07 acute sinusitis > amoxicillin 875 BID 7 days
04/29/07 well woman exam > Gardisil, Yasmin
09/02/07 diabetes, A1C 8.2, start metformin 500 BID

The next layer down, the "Executive Summary", is what I would communicate to a surgery consultant. It is a 3-4 sentence description of this encounter in a depth adequate for a consultant or other peer not needing a complete picture of this patient.
For example, it might say "57 year old type 2 diabetic recently started on metformin with good control, needing evaluation of chronic cough, not on an ACE inhibitor".

Next, the 3rd layer, the "Working Layer" is the layer clinicians would like to work in for the details they need. That is, before we started documenting to cover our assess.
It would include only the pertinent history elements necessary to understand the diagnosis and treatment. In the Review of Systems, it would only include the positive elements, with a few negatives (e.g. "no murmur" if that is pertinent to note).
In the Assessment and Plan, only the parts that are not assumed. I do need to know which antibiotic was used. I don't need to read that the patient was told to take tylenol and come back if they don't get better as expected.

The fourth layer would make my attorney, my risk-manager, and my chart reviewers happy. All the wealth of detail is there that would only annoy the rest of us. All the detail that makes my record look more like a contract, and less like a story about a person.
Parenthetically, there are layers deeper than these four. These layers include the security/audit trails that record who recorded what and when. We'll ignore them for our purposes here.
So, how do we bring this concept about?
Your thoughts?